Advanced Endodontics
Root Canal Therapy
The Pragmatic Approach to Tooth Retention
1. Clinical Overview: Pragmatic Preservation
In our clinical practice, we strictly reject the concept of ‘heroic’ dentistry—the stubborn attempt to save a biologically ruined tooth that ultimately risks a patient’s time, finances, and bone health on a failing foundation. We view Root Canal Treatment (RCT) as a highly targeted, predictable solution only for cases where the vast majority of the coronal tooth structure remains healthy, intact, and structurally sound.
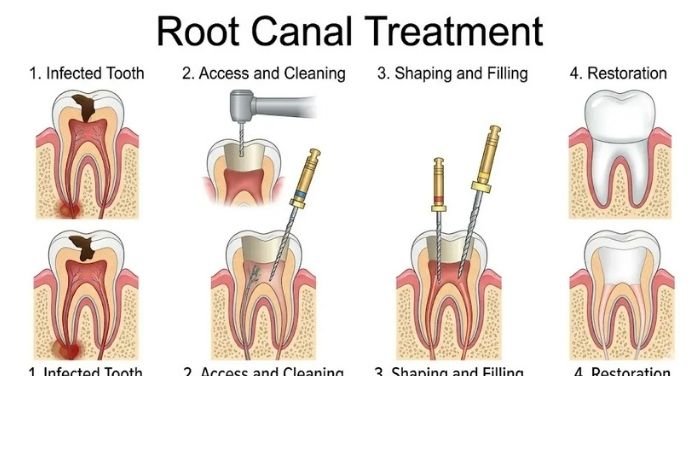
2. The Procedure Protocol
Our modernized endodontic workflow intensely focuses on advanced mechanical efficiency and absolute biological cleanliness to resolve pulpal necrosis and periapical infection rapidly and predictably.
Instead of relying blindly on tactile feel or repetitive, high-radiation 2D X-rays, we deploy micro-computerized electronic apex locators. This advanced impedance technology allows us to mathematically determine the exact biological end of the root (the apical constriction) to within 0.5mm, guaranteeing we clean the entire infected canal without inadvertently perforating and irritating the sensitive surrounding jawbone.
We utilize sophisticated, high-torque, microprocessor-controlled rotary motors to expertly excise the infected nerve tissue. By heavily focusing on efficient, continuous-taper canal shaping, we drastically reduce the fatiguing time the patient spends in the chair while ensuring the root is geometrically prepared to perfectly receive a dense, hermetic, 3D seal.
3. Candidacy: The “Restorability-First” Filter
The most critical phase of our RCT protocol happens entirely before we ever pick up a surgical handpiece. We actively deploy a rigid “Restorability-First” diagnostic filter to fiercely protect our patients’ financial and biological outcomes.
We rigorously inspect the tooth for a minimum of 2mm of sound, 360-degree tooth structure remaining solidly above the bone crest. If the decay has tunneled too deeply into the root, the lateral “leverage” generated by chewing forces will inevitably snap the brittle tooth off at the gumline, rendering the root canal a complete failure.
If more than 50% of the natural clinical crown is destroyed by caries or fracture, we halt the endodontic process. We then initiate a serious, transparent conversation about whether an extraction and immediate titanium implant is the overwhelmingly more “biological” and financially sound choice for the patient’s long-term health span.
4. Recovery: Buying Time vs. Permanent Fix
We are relentlessly transparent with our patients: a root canal is a phenomenal, highly engineered way to chemically retain your natural “equipment,” but it forever alters the biology of the tooth.
Once the infected nerve and vascular tissue are surgically excised, the tooth permanently loses its internal hydration and blood supply. This dentinal desiccation means the tooth acts somewhat like a dead branch on a tree—it becomes highly brittle and structurally vulnerable over time without proper reinforcement.
By strictly limiting RCT exclusively to cases presenting with robust, healthy surrounding bone and mathematically adequate coronal tooth structure, we actively avoid the chronic, lingering “soreness” notoriously associated with failing root canals. The vast majority of our patients experience minimal post-op nociception (pain) and return to uninhibited, normal function almost immediately, provided the tooth is properly crowned.
5. Tech Specs: Modern NiTi & Tapered Sealing
When the biological case successfully passes our rigorous diagnostic filters, we execute the therapy utilizing advanced materials specifically engineered for operational speed, safety, and apex integrity.
We deploy ultra-flexible, heat-treated Nickel-Titanium (NiTi) rotary files that possess profound shape memory, allowing them to perfectly follow the complex, tortuous curves of the root canal without stripping the walls. Furthermore, by employing a strict, zero-compromise single-use protocol (opening fresh, sterile files for every single case), we eliminate cyclic metal fatigue and virtually eradicate the catastrophic risk of instrument separation (breaking a file inside the root).
We match the terminal obturation filling material exactly to the engineered taper of our final rotary files. This precision “master cone” fit guarantees that the empty canal is completely obliterated with a dense, biocompatible, rubber-like material, establishing an impregnable apical seal that totally prevents bacteria from re-colonizing the empty pulpal space.
6. The Science of Stability
Why the Crown is the True Hero
An immaculate endodontic treatment is completely meaningless if the coronal seal on top of it structurally fails. Coronal microleakage will doom any root canal. In our practice, the RCT and the final restorative crown are treated as a single, inseparable mechanical unit.
Because desiccated, endodontically treated teeth are highly prone to devastating vertical root fractures via cuspal flexure, we absolutely mandate “cuspal coverage.” By cementing a full-coverage ceramic crown or a high-strength onlay immediately, we physically ferrule and brace the fragile tooth against the 200+ lbs of shear pressure generated during daily mastication.
We operate with total clinical realism: we educate our patients that if a complex root canal eventually fails due to recurrent infection or unseen micro-fractures, we already have an infallible “Plan B” (the extraction and titanium implant) fully mapped out. However, by strictly utilizing our “Rule of 50” to select only the absolute best biological candidates for RCT, we ensure that “Plan B” remains a highly distant safety net rather than an immediate, tragic necessity.