Advanced Periodontal Surgery
Socket Preservation
The “Stabilized Shield” Grafting Protocol
1. Clinical Overview: Site Preservation vs. Bone Collapse
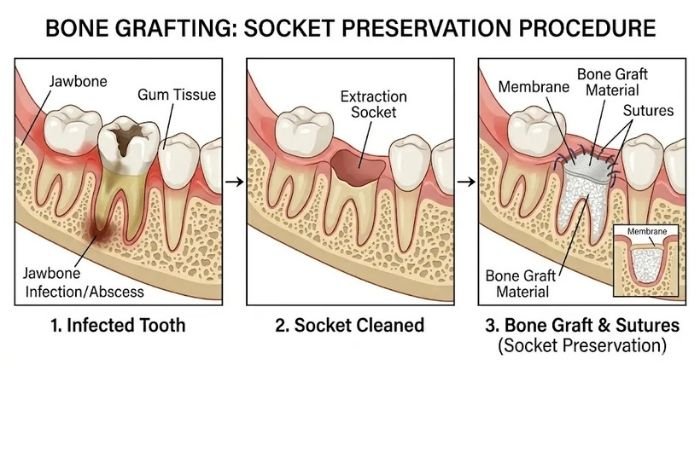
When a terminal tooth is extracted, the body initiates a profound biological response: it naturally and rapidly begins to resorb the surrounding alveolar bone because the bundle bone no longer serves a mechanical purpose. At DayOne Dental, we absolutely do not wait for this catastrophic volumetric collapse to happen.
Our surgical practice focuses heavily on proactive Socket Preservation—filling the extraction void immediately to mechanically and biologically “freeze” the hard tissue architecture in place. This intervention isn’t merely about filling a hole; it is about maintaining the critical surrounding buccal and lingual bone to ensure neighboring teeth are not structurally compromised. By performing Guided Bone Regeneration (GBR) at the exact time of extraction, we successfully help patients avoid dramatically more invasive, painful, and expensive “autogenous block grafts” or sinus floor elevations down the road.
2. The “Stabilized Shield” Philosophy
A particulate bone graft is entirely dependent on, and only as good as, its mechanical stability. Micromotion is the absolute enemy of bone regeneration.
3. The Procedure Protocol
The Sub-Gingival “Envelope” Technique: Our surgical workflow intensely focuses on the absolute mechanical immobilization of the bone graft through two highly critical, operator-sensitive steps:
Immediately after the terminal tooth is carefully elevated and removed, we utilize specialized micro-instruments to create a tiny 3mm sub-periosteal “pocket” (a partial-thickness envelope flap) entirely under the mucosal gums surrounding the socket. We strategically slide the resorbable membrane deep into this pocket, effectively “tucking” it in like a tight bedsheet over the graft.
We execute a highly precise suturing technique (most often a continuous criss-cross or figure-eight tension suture) to lock the membrane in place beneath the tissue. This guarantees the underlying graft particulate cannot suffer micro-movement or dislodge—which is overwhelmingly the #1 biological cause of graft failure in traditional, unprotected “open” extraction sites.
4. Candidacy & Diagnostics: Mapping the Walls
The clinical success of a “tucked” sub-gingival membrane depends heavily on the pre-existing integrity of the surrounding host bone walls.
Patients possessing inherently thin “buccal plates” (the ultra-fragile front wall of the facial tooth socket, common in anterior teeth) who are at an astronomically high risk for catastrophic bone collapse post-extraction.
We utilize ultra-low-dose 3D CBCT imaging to accurately check the height, thickness, and Hounsfield density of your bone walls. If a cortical wall is absent (a dehiscence), our “tucking” technique becomes absolutely vital, as the membrane physically acts as the artificial “wall” your body requires to predictably rebuild the lost structure.
5. Recovery: Preventing the “Bone Melt”
The clinical “nerd” secret to our exceptionally high regenerative success rate is the principle of Cellular Exclusion.
Biologically, bone-building cells (osteoblasts) are incredibly slow to migrate; conversely, gum-tissue cells (fibroblasts) are exceptionally fast. If they “race” into an open socket, the rapid gum cells win every single time, leading to fibrous encapsulation and “mushy” non-integrated bone. Our tucked membrane acts as an impenetrable “bouncer,” aggressively keeping the epithelial gum cells out for 4 to 6 months while the slow-moving bone safely solidifies and matures underneath.
Because the highly engineered membrane is strictly tucked and securely sewn, the surgical site is fundamentally “closed” and isolated from the hostile, bacteria-rich oral environment. This deliberate primary-intention healing protocol significantly reduces the pathological risk of alveolar osteitis (“dry socket”) and post-operative infection, leading to a much smoother, painless, and infinitely more predictable healing phase.
6. Tech Specs: Site-Specific Regeneration
We vehemently reject cheap, “quick-dissolve” barrier materials that prematurely disappear before the intense biological job of bone turnover is complete. Our protocol is strictly built on a “Right Material, Right Site” strategy to ensure that the graft resorbs only when the host bone is fully vascularized and ready to take over.
A. Strategic Bone Selection: Scaffold vs. Signal
We do not believe in a lazy, one-size-fits-all approach to bone grafting. We select biomaterials based entirely on the specific anatomical requirements of the defect.
In these severe “open-faced” structural defects, we utilize Raptos® Mineralized Allograft. These osteoconductive particles act as high-strength, slow-resorbing “bricks,” providing the dense mineralized scaffold necessary to physically prop open and maintain the ridge width where a vital cortical wall is entirely missing.
When the bony housing is fully intact, we prioritize speed and cellular vitality by deploying DBM 100 Putty. This highly osteoinductive material provides the intense biological protein “signal” (BMPs) needed to actively jumpstart rapid bone turnover and angiogenesis within the protected environment of the enclosed socket.
B. Advanced Membrane Barriers: Protection by Design
The membrane is the ultimate “guardian” of the graft. We select our specific barrier profiles based on the required longevity and complexity of the surgical repair.
For standard 4-wall socket preservation, we deploy Snoasis BioXclude. This advanced amnion-chorion “biological bandage” allows for safe non-primary closure, adhering naturally to the moist site to protect the underlying particulate while chemically accelerating the migration of new, healthy gum tissue directly over the top.
To surgically repair a dehiscence or fenestration, we must utilize Neomem® FlexPlus. This highly specialized, cross-linked porcine collagen is chemically designed to resist enzymatic breakdown and last 16–28 weeks, perfectly matching the natural, slow clock of bone maturation. Its high drapability allows us to seamlessly “shrink-wrap” the defect, while its immense tensile strength ensures it stays securely sutured in place without tearing.
C. Suture Bio-Compatibility & Stability
Braided silk sutures act like sponges. We entirely reject them. Instead, we utilize high-tensile, non-wicking monofilament sutures (such as PTFE) that biologically cannot “pull” or siphon bacteria from the dirty oral cavity down into the sterile surgical site. This critical material choice maintains a pristine, uncontaminated healing environment beneath the soft tissue surface throughout the entire multi-month integration period.